Chondrosarcomas are bony tumors that occur mainly in the pelvis, hip or shoulder and rarely in the skull. Headache, double vision, hearing loss or tinnitus are among the most common symptoms of chondrosarcomas of the skull. Therapy consists primarily of maximal microsurgical resection, with concomitant radiotherapy also playing an important role.
Clinical significance
Chondrosarcomas are rare, malignant bone tumors that arise from cartilage tissue. They mainly affect the pelvis, hip or shoulder. Only 2 % of all chondrosarcomas grow at the base of the skull. They account for 0.1–0.2 % of all intracranial tumors and only 6 % of all tumors of the skull base. Chondrosarcomas grow slowly but destroy bone in the process and metastasize early.
The World Health Organization classifies intracranial chondrosarcomas into WHO categories I to III depending on malignancy. A large proportion of the chondrosarcomas described in the literature (90 %) belong to WHO categories I (50 %) and II (40 %), which explains the generally good prognosis for this type of tumor.
Who is most likely to develop chondrosarcoma?
Chondrosarcoma is the second most common type of bone cancer, accounting for around 20 % of all cases. Chondrosarcoma predominantly affects people between the ages of 40 and 70. The tumor is found almost equally often in men and women (women : men = 1.1 : 1) *. A higher incidence rate of this disease is seen in patients with Maffucci syndrome or Ollier disease.
What symptoms does chondrosarcoma cause?
The symptoms are mainly due to the location of the tumor and the associated local compression or infiltration. These are the general symptoms:
- Headaches
- Double vision
- Hearing loss
- Tinnitus
- Cranial nerve deficits
How is chondrosarcoma diagnosed?
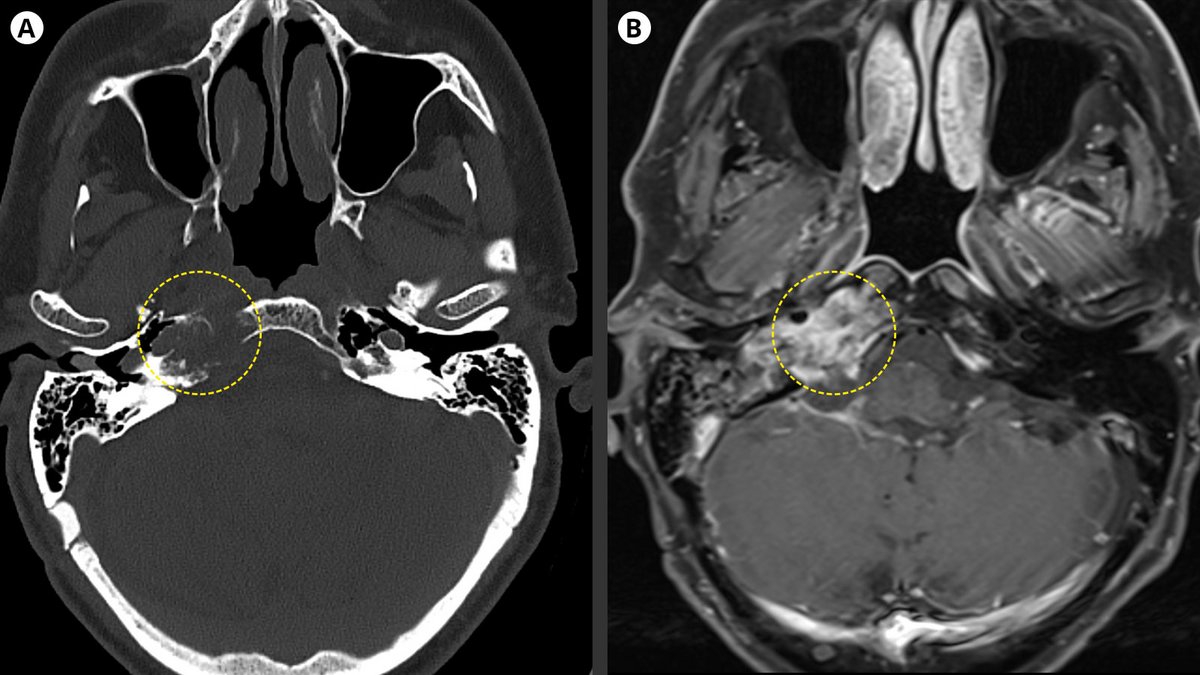
The suspected diagnosis is made by imaging to clarify symptoms or as an incidental finding in the course of other diagnostics. On computed tomography (CT), chondrosarcomas present themselves as bone-eroding lesions and often show calcifications. Magnetic resonance imaging (MRI) reveals possible "honeycomb" patterns of the tumor. Due to the radiological characteristics, chordomas should be considered in the differential diagnosis. However, a definitive diagnosis can only be made after tissue sampling and fine-tissue microscopic examination by a neuropathologist.
What are the treatment options?
Microsurgery
The primary therapy consists of maximum, gentle microsurgical tumor removal. For this purpose, depending on the location of the tumor, the latest procedures such as neuronavigation and intraoperative neuromonitoring are used, which enable the neurosurgeon to work with the highest precision and safety under the operating microscope.
Radiotherapy
Complementary radiotherapy is a recognized treatment option that improves both tumor-free interval and survival rates. The following options are distinguished:
- Photon therapy
- Stereotactic radiosurgery
- Proton therapy
Chemotherapy
Chemotherapy does not play a major role in the treatment of chondrosarcoma.
Why you should seek treatment at Inselspital
We seek the optimal treatment strategy for each individual patient. This is done in our certified neuro-oncological tumor center by an interdisciplinary team. This tumor board, which meets weekly, is composed of specialists from neurosurgery, neurology, neuro-oncology, nuclear medicine, radio-oncology and pathology. Here, each patient is discussed individually in order to determine the optimal treatment options for him or her.
For the operation itself, we use innovative technical procedures such as neuronavigation and intraoperative neuromonitoring, which was developed at Inselspital. These new achievements are a guarantee for maximum precision during surgery and maximum safety for our patients.
-
van Praag Veroniek VM, Rueten-Budde AJ, Ho V et al. Incidence, outcomes and prognostic factors during 25 years of treatment of chondrosarcomas. Surg Oncol. 2018;27:402-408.